

TLDR
- Document control is a patient safety issue, a litigation risk and a regulatory obligation.
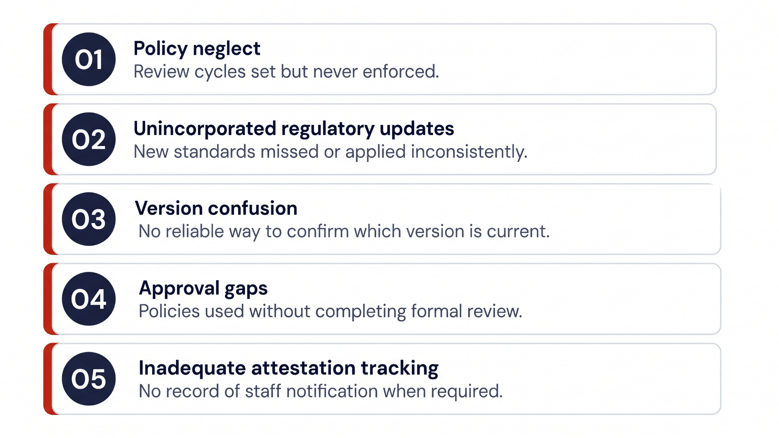
- The most common failures follow predictable patterns: policy neglect, version confusion, missed regulatory updates and approval gaps.
- High-reliability organizations don't wait for a survey to find them.
- They build systems that surface gaps before they cause harm.
Healthcare leaders invest significant effort in patient safety. They build safety committees, run failure mode and effects analyses, develop staff education programs and track adverse event data. These are the right instincts. But one area that often gets overlooked in that risk calculus is document control, and the gaps it creates carry real, compounding consequences for clinical outcomes, regulatory standing and legal liability.
This post examines why document control is a patient safety issue, what foreseeable risks emerge when it is mismanaged and what it takes to build a governance foundation capable of supporting a high-reliability organization.
What document control means in healthcare.
Document control is the structured process by which a healthcare organization creates, reviews, approves, distributes and retires its official policies, procedures and clinical guidelines. It is the mechanism that ensures the policies staff use to guide care decisions are current, accurate and sanctioned by leadership.
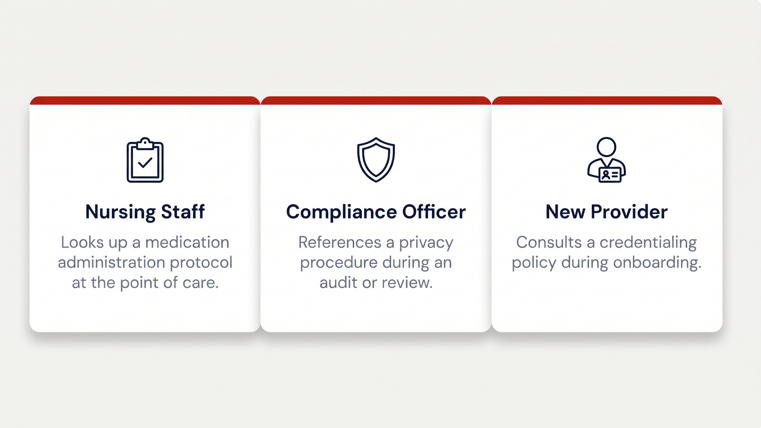
In a healthcare setting, document control is not a back-office function. It directly affects what happens at the point of care.
When it does not, the effects are rarely isolated.
A single outdated policy can generate inconsistency across an entire department. A missed regulatory update can expose an organization to accreditation findings or enforcement action. A document that never made it through proper approval can become evidence in litigation.
Document control as a patient safety issue.
Most healthcare organizations have well-developed frameworks for clinical risk management. What is less common is treating document control as a direct component of that framework, even though the connection is clear.
When staff operate from outdated or unapproved clinical guidelines, the risk of adverse events increases. When conflicting versions of a policy exist across departments, care becomes inconsistent. When a policy has not been reviewed against current evidence-based practice, it may direct staff toward approaches that are no longer clinically appropriate.
The Joint Commission has long identified communication failures as a leading root cause of sentinel events. While communication breakdowns take many forms, inconsistent or inaccessible policies are a systemic contributor, one that proper document control directly addresses.
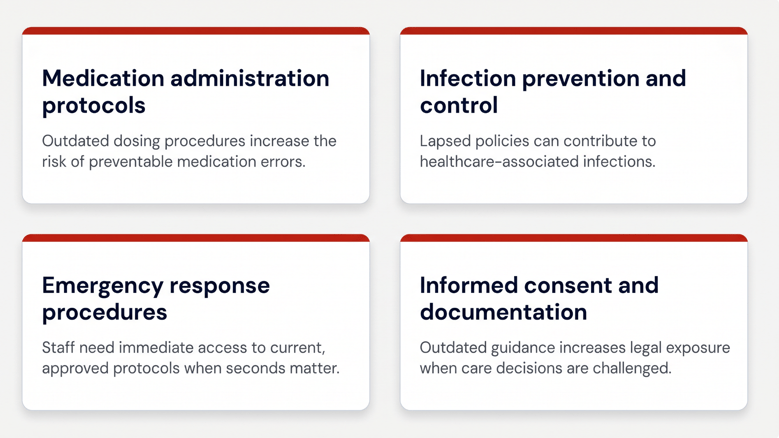
Patient safety risk related to document control surfaces most acutely in areas like:
The litigation dimension.
One aspect of document control that deserves more attention is its role in litigation. When an adverse patient care event occurs, legal discovery typically includes a review of the organizational policies in effect at the time of the event.
This creates a specific kind of foreseeable risk: if your document control practices cannot demonstrate that staff had access to current, approved, evidence-based policies, and that those policies were reviewed on a defined schedule and updated in response to regulatory changes, the organization's position in litigation becomes significantly more difficult.
When policy neglect is documented such as missed review cycles, unincorporated regulatory changes and policies that were never formally approved, that evidence of negligence becomes discoverable.
This is why document control is not simply an operational concern. It is a risk management obligation, and healthcare compliance and legal teams should be as invested in it as clinical leadership.
Regulatory and accreditation requirements.
Regulatory agencies set explicit expectations for document control that go beyond good practice; they are standards organizations are evaluated against.
The Joint Commission requires that organizations maintain policies and procedures that reflect current standards of care, are approved by appropriate authority and are accessible to staff. Surveyors assess not just whether policies exist, but whether they are current, consistently applied and supported by a review process. Gaps in any of these areas can result in Requirements for Improvement or, in more serious cases, Immediate Threat to Life findings.
CMS Conditions of Participation similarly require that hospitals maintain written policies governing patient care services and that those policies be reviewed and updated at defined intervals. OSHA mandates written safety programs and procedures for specific hazard categories, including bloodborne pathogen exposure, hazard communication and respiratory protection. HIPAA requires documented privacy and security policies with defined training and enforcement processes.
Meeting these requirements on paper is one thing. Demonstrating them under survey conditions with a complete audit trail, version history and staff attestation records is another. Organizations that rely on manual processes, shared drives or decentralized document management often find that gap during surveys, not before.
Common failures in healthcare document control.
Understanding where document control breaks down helps organizations identify their own exposure. The most common failures follow predictable patterns.
The path to high-reliability document control.
A high-reliability organization (HRO) operates with a preoccupation with failure, meaning it actively looks for and addresses the gaps that could lead to harm before those gaps manifest in adverse events. Effective document control is foundational to that mindset.
HROs do not wait for a survey finding or a litigation event to identify document control failures.
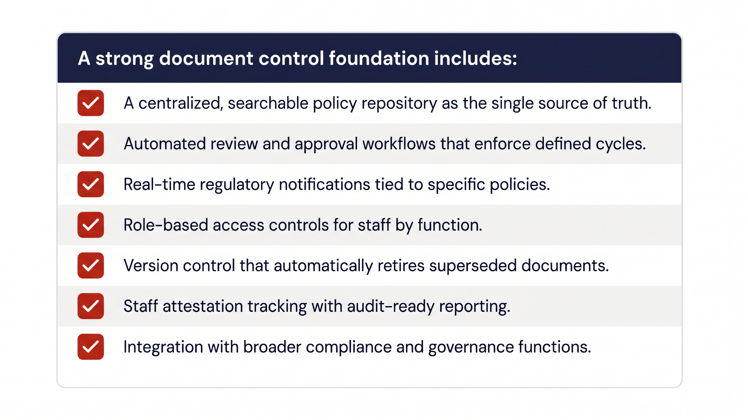
They build systems that surface gaps proactively: review cycles that are enforced automatically, regulatory change monitoring that triggers policy updates, version control that makes it impossible to distribute an unapproved document and attestation tracking that shows, in real time, which staff have acknowledged which policies.
Getting there requires moving away from manual, decentralized processes and toward a purpose-built policy management infrastructure.
What a strong document control foundation looks like in practice:
Why healthcare-specific tools matter.
Generic document management platforms can store and organize files. What they cannot do, at least not without significant customization, is reflect the regulatory logic of healthcare.
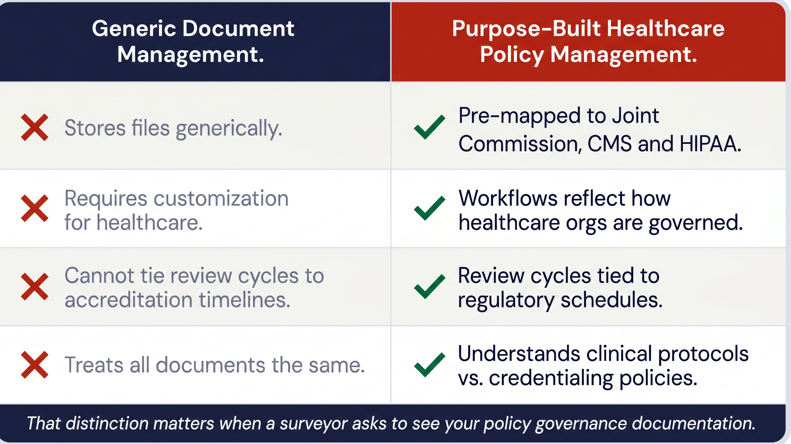
Purpose-built healthcare policy management software does. It is designed by people who understand the regulatory environment healthcare teams operate in, which means the workflows, templates and controls already reflect how healthcare organizations are actually governed, not how a generic enterprise system assumes they work.
That distinction matters when a surveyor asks to see your policy governance documentation. It matters when your legal team is responding to a discovery request. And it matters every day that your staff rely on your policies to guide safe, consistent care.
Closing the gap before it becomes a liability.
Document control is not the most visible part of healthcare governance, but it is one of the most consequential. Organizations that treat it as a low-priority administrative function are accepting a level of foreseeable risk that patient safety, compliance and legal considerations do not support.
The good news is that the gap is closeable with the right infrastructure, the right workflows and a clear understanding of what is at stake.
Explore Ntracts' healthcare policy management software or request a personalized demo to see how purpose-built policy governance supports safer, more compliant healthcare operations.
Sources
- The Joint Commission: Sentinel Event Data (jointcommission.org)
- HIPAA Journal: "At Least 43% of Covered Entities Still Not Using Software for HIPAA Compliance Tracking," Nov. 28, 2024
- CMS Conditions of Participation: Hospital (42 CFR Part 482)
- OSHA: Bloodborne Pathogens Standard (29 CFR 1910.1030)


